Evolution of Medical Records, development and its importance
History
The history of medical records runs parallel with the history of medicine. Records are as necessary for the practice of medicine as medications are for effective treatment and they can be traced back to ancient times. The earliest records were primitive in form and very different from present medical records, but they served to record medical achievements for later generations. As time went on, medical records became more detailed and in Egypt, Greece and Rome physicians wrote important medical and surgical treatises.
I. Egyptian period
It is characteristic of earliest historical times that great achievements by men were ascribed to a god. In Egypt, mediating power between god and evil furnishes a good example of this.
The first real physician of record in Egypt is Imhotep. He lived in the Pyramid Age and was a grand vizier, chief architect, and royal medical adviser to a pharaoh of the twenty-ninth century before Christ.
II. Greek period
Greek medicine was not purely Grecian, but was influenced by contributions from older civilisations, especially those of Egypt, Babylonia, and Assyria.
- This in no way reduces the credit to the Greeks for introducing the scientific spirit into the art of healing, but merely indicates the various sources from which they were able to draw information.
Both the Greeks and Romans with the Egyptian Imhotep, as was said previously, equated Aesculapius. He is probably the most venerated physician of all times. As with Imhotep, it will probably never be definitely established whether he was a man or myth However, there is evidence of such a Physician who was widely recognized throughout Greece, and even in Egypt. He is credited with curing many who were so ill that they not expected to survive.
It was on the Greek island of Cos near Asia Minor that Hippocrates, known as the “Father of Medicine”, was born about 460 B.C. As his forefathers had done before him, he drew the rudiments of his medical knowledge from the reports of cases collected in the Aesculapium at Cos In the nineteenth century, the famous Massachusetts General Hospital, Boston, Massachusetts, was opened. It has the distinction of having a complete file of clinical records, with all cases catalogued; dating from the day it was opened.
- Before the end of the year 1897 a librarian had been employed and the care of clinical records, including their cataloguing became a part of her work. This hospital seems to be the first to have had a medical record librarian. She was Mrs. Grace Whiting Myers who was the first president of the association of Record Librarians of North America and honorary president of the American medical record Association.
- The first hospital records written in ink are legible to this day. Hospitals were keeping records as a fashion prior to the twentieth century; it was not until the beginning of this era that medical records received serious attention by other types of hospitals, and especially by medical and hospital associations
In 1905 the physicians themselves began to give some thought to the value and necessity of adequate medical records
The history of medical records, from the earliest beginnings to the present time, has continued unbroken, even though greater progress has been made in some periods than in others.
The greatest improvement began with the inauguration of the hospital standardisation movement in 1918, and new gains were made after organisations of the medical record workers and implementation of the medicare regulations.
Development of medical records
The skills of many medical and allied health specialists are required to provide complete care to the patient. The team consists of physicians, nurses and numerous allied health personnel.
They inform and advise each other through their entries in the records about their findings, observations, opinions and treatment of the patient.
Good medical care generally means a good medical record, while an inadequate medical record may reflect poor medical care.
Medical records store information concerning the patient and his care. To be complete, the medical record must contain all relevant details to clearly identify the patient, to support the diagnosis, to justify the treatment, and to record the results accurately.
A written medical record must be maintained on every person who has been admitted to hospital or other health care facility. This may be an out- patient, in-patient or emergency patient.
The medical record usually begins in the patient registration area with the patient’s registration. It is there that the essential identification data and other necessary information are obtained.
This new record usually accompanies the patient to the vision room. The attending physician and his co-workers add their notes. These include the patient’s complaints regarding the onset and course of present illness, his personal/family history, a complete report of the physical examination, and a plan for study and treatment in the hospital.
Additional reports are added as they are made. These include laboratory, X-ray reports, in-patient reports when a patient gets admitted, reports of operation as written or dictated by the surgeon, and reports of the paramedical services .
The nurses record all observations, medications, treatments and other services rendered.
The attending surgeon records the progress of the patient in the progress notes as often as necessary for an adequate report until discharge of the patient.
When the patient is discharged, the patient’s care is summarised by the attending surgeon or his designee in the discharge summary, which includes the patient’s condition upon discharge and pertinent instructions for care following hospitalisation.
Uses of medical records
The medical record contains information acquired in a doctor - patient relationship, which is generally considered to be confidential. The hospital is responsible for preventing access to patient’s medical record by non-authorised persons from the time the medical record is initiated, during hospitalisation, as well as after discharge. Identification data unrelated to treatment are generally considered non-confidential and may be released without the consent of the patient. Release of this information, however, should be carefully screened and given out only in response to proper enquiry.
Medical records are used
- To record the patient’s problem, history, and treatment given either as out-patient or in-patient
- To form a bridge between the doctors and other paramedical professionals contributing to patient care
- To give continuity in treating the patient during subsequent visits or admission
- To assist in protecting the legal interests of the patient, the hospital, and the doctors
- To provide data for any research, study or education
- To review the quality of treatment given by doctors, nurses and other paramedical professionals
- To provide data for any third party agencies connected with the patient, doctor and hospital
Value of the medical records
The content of records may not only aid in diagnosis of a specific case, but may aid in the treatment of another case, and it is also of legal value. The medical record is an orderly written report of the patient’s complaints, the diagnostic findings, treatment, and end results. In total they form a clinical picture and, when completed, contain sufficient information to clearly identify the patient, to justify the diagnosis and treatment, and to record results because, “Patient forgets and records remember”. “The record is of value to the patients, the hospital, the physician, and for research and teaching” (Fig.1.1).
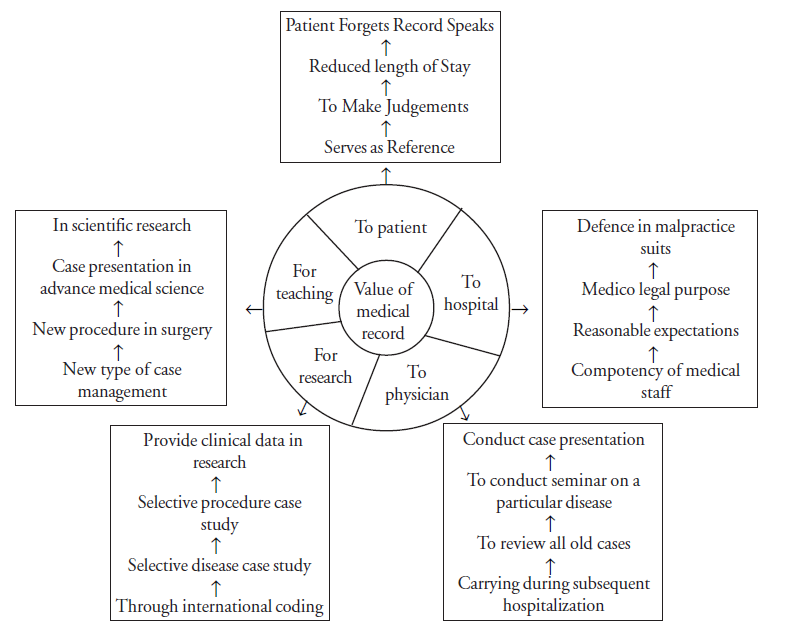
i. For patient
- A complete report of an illness results in the accumulation of a large amount of information about the patient
- Physicians cannot be expected to remember the details of each patient’s illness. Therefore, medical records serve as a reference
- When a patient requires subsequent hospitalisations with the same or another illness, and with or without a change of physician, the medical record of the previous hospitalisations will enable the physician to review and analyse the previous illness and treatment and make judgements as to the course of treatment to be followed.
- With this knowledge of the patient’s previous hospitalisation the physician may be able to initiate treatment without waiting for results of diagnostic tests
ii. For hospital
- The medical record is of value to the hospital in evaluating the competency of the medical staff and the end results of treatment
- Unless an accurate record is kept, neither the hospital nor the physician can justify the results of treatment
iii. For the physician
- Medical record will be useful to a physician when he needs to gather information during subsequent hospitalisation
- In addition a physician may wish to know how many times he has been called in consultation during a given period
- The hospital as well as the physician may need the record for medico legal purposes.
iv. For scientific research and teaching
- In scientific research the medical record is indispensable. Case studies supply a practical and reliable source of material for the advancement of medical science.
- In addition, the medical record is valuable in all teaching programs. It is a source document for medical facts related to disease, treatment, care and results.
- Without the documentation of patient care found in the medical record, payment for services could not be justified.
Summary
The history of medical records, from the earliest beginnings to the present time, has continued unbroken, even though greater progress has been made in some periods than in others. The mid-twentieth century brought in an era in which all medical, paramedical, and hospital associations are united in the same primary goal-to take proper care of the sick and injured. A medical record must be maintained on every person who has been admitted to the hospital as an in-patient, out-patient, or as an emergency patient. The medical record, documents the hospital experience of the patient. Other purposes are to serve as a basis for continuity in the evaluation of the patient’s condition and treatment, to assist in protecting the legal interests of the patient, the hospital, and the doctors, and to provide data for use in research and education.
Key points to remember
- The earliest records were primitive in form and very different from the present medical records, but they served to record medical achievements for later generations
- Mrs. Grace Whiting Myers was the first president of the association of Record Librarians of North America and honorary president of the American Medical Record Association.
- A medical record must be maintained on every person who has been admitted to the hospital as an in-patient, out-patient, or as an emergency patient.
- The content of the medical record is developed as a result of the interaction of the members of the healthcare “team” who use it as a communication tool.
- The purpose of medical records is to serve as a basis for continuity in the evaluation of the patient’s condition and treatment.
- Medical records are useful in protecting the legal interests of the patient, the hospital, and the doctors, and to provide data for use in research and education.
Teaching suggestions
- Explain the medical records assistants to understand how medical records came into existence during the Egyptian, Greek and Greco-Roman periods.
- Demonstrate the values of medical records to the hospital, patients, and physician through OHP presentation.
- Show the diagnostic and surgical coding data and explain how it is useful to the hospital and third parties.
Student exercise
Answer the following
1. Identify the following persons or organisations:
- The first medical record librarian.
- The first Egyptian physician of record.
- The god of letters.
- The “Father of Medicine.”
2. Trace the history of medical records through the Egyptian, Greek, and Greco-Roman periods.
3. Identify six uses of medical records.
4. Discuss the value of medical record to each of the following:
- The patient
- The physician
- The hospital
5. Describe the development of medical records in the hospital.