Basic Knowledge of Sutures, Needles and Lenses
Different types of sutures, needles and lenses are used in eye surgery. The OA should have knowledge about the different types of sutures, needles and lenses, so that they can assist the surgeon during the surgery effectively.
Suture and needles
A suture is a length of thread with a needle attached to one (single-armed) or both ends (double-armed). In ophthalmic surgery it is common for doublearmed sutures to be used. (Example: cataract and cornea surgery) A length of double- armed suture material is cut in half. The unused suture lengths can be re-sterilized by soaking in spirit or by E.T.O sterilisation. (Fig 7.1)
Sutures are used in extra capsular cataract surgeries,conjunctival suturing, corneal tear, repair corneal transplants, filtering procedures, squint surgeries, scleral buckling, retinal surgeries etc..
SutureSuture materials have been developed enormously over the past 20 years. Surgeons and manufacturers work closely together in making different types of suture materials suitable for various parts of the body.
Types of suture- - Non-absorbable
- - Absorbable
- - Nylon
- - Braided silk
- - Virgin silk
- - Polyester
- - Poly propylene
- - Ethicon (polyglycolic acid suture)
- - Chromic catgut
- - Collagen
- - D and G (Dexon)
Non-absorbable sutures such as (5-0) or (6-0) mersilene or dacron are used in muscle procedures involving the obliques or rectus muscles. For e.g., they are used for joining the muscle bellies in muscle transposition procedures. Non-absorbable sutures may also be used for anchoring supramid sheets,sleeves or caps. The 4-0 or 5-0 black silk suture passed through the limbus is useful for stabilising and retracting the eye during surgery. This suture is also useful as a traction suture to fix the globe in a given position for several days postoperatively in cases where surgery is performed to correct mechanical restrictions. Non- absorbable sutures remain in the tissues.They don’t get absorbed and must be removed once the wound has healed. After several years even nonabsorbable sutures may degrade. These can be monofilament, twisted or braided.
a. MonofilamentA single strand (Example: Nylon). It can become untied easily, so requires firm knotting. It runs smoothly through tissues.
b. TwistedTwo or more strands twisted around each other (Example: Virgin silk), knots easily but does not run smoothly through the tissues.
c. BraidedTwo or more strands plaited together, knots easily but does not run smoothly through the tissues. They are not advisable when there is infection. (Example:Silk)
Absorbable sutureAbsorbable sutures – (catgut or collagen, plain or chromic) have replaced silk sutures for extra ocular muscle surgery. The sutures vary in size from 4-0 to 6-0. Catgut differs from collagen that it is made from a single sheep intestine, which is composed of 95%collagen and 5%noncollagenous –associated tissue. Collagen sutures are formed by an extrusion of homogenized, pooled beef fascia and are 100% collagen.
NeedlesOphthalmic needles are made of stainless steel and are swaged to the suture material for smooth passage through tissue.
The safest needles for extra ocular muscle surgery are the fine spatula type. The spatula needles cut tissue at its tip and sides only and actually displace tissue above and below. This displacement results in less chance of inadvertent scleral perforation, provided the flat of the spatula is parallel to the sclera.
Curved cutting and reverse cutting needles should be used with caution and should be of very fine caliber. A reverse cutting needle is available on the (4-0) black silk, which is frequently used for placement of traction sutures. Extra care should be taken when using the large needle.
Needles for special application are available. These include short, heavy needles for posterior fixation suture. Some prefer a long fine needle that is supplied by Ethicon for the crossed swords technique; others prefer a moderate length fine wire. (0.203mm diameter) spatula needle for muscle reattachment and a smaller half circle needle for conjunctival closure. The heavier needle (0.330 mm wire diameter) on 5-0 vicryl is used for ptosis surgery.
Types of needles- - Spatula
- - Taper point
- - Reverse cutting
- - Conventional
A rhomboid-shape in cross section with two- sided cutting edges used in the cornea and the sclera where the plane of penetration must be precise.
Taper pointA cone-shaped, single point needle with a round shaft used for delicate tissues
Reverse cuttingTriangular in cross section with two- side cutting edges and a lower cutting edge used passing through for resistant tissue.
Conventional cuttingTriangular in cross section with two - side cutting edges and an upper cutting edge. (Largely replaced by the reverse-cutting needle.)
Needles also come in different diameters, usually to match the diameter of the suture material to which they are attached.
Needle / diameter sizes110mm, 150mm, 200mm, 230mm, 250mm, 280mm, 330mm, 430mm.
Needle manufacturing process- - Wire cutting
- - Pressing
- - Channeling
- - Grinding
- - Deburring
- - Attaching
- - Curving
- - 1/2 circle
- - 3/8 circle
- - 1/4 circle
(Example: 6402N)
- - 6-wire size
- - 4-140 angle curvature
- - 0- (10-0) suture
- - 2-Double arm
- - N-Nylon
8482S
- - 8-wire size
- - 4-140 Angle curvature
- - 8-8-0 Suture
- - 2-Double arm
- - S-Silk
Intraocular lenses
Surgical removal of cataract and the implantation of an intraocular lens is one of the most successful microsurgical procedures today.
HistorySir Harold Ridley was the first person to successfully implant an IOL in the eye. He did this on november 29, 1949 at St.Thomas hospital, London. While working with RAF casualties during World War II,
Ridley noticed that when splinters of Perspex from aircraft cockpit canopies became lodged in the eyes of wounded pilots, they did not trigger infection or reaction. These observations lead him to propose the use of artificial lenses in the eye to treat cataracts.
He went on to develop comprehensive programmes for cataract surgery with intraocular implants and pioneered this treatment in the face of prolonged strong opposition from the medical community. He worked hard to overcome complications, and had refined the technique by the late 1960s. With his pupil Peter Choyce he eventually achieved worldwide support for the technique, and the intraocular lens was finally approved for use in the USA by the Food and Drug Administration in 1981. It is now the most common type of eye surgery. There are a number of ways a cataract can be removed.
These are:- - Intracapsular cataract extraction
- - Extra capsular cataract extraction
- - Phacoemulsification
Commonly used 30 years ago, intra-capsular cataract extraction, or ICCE, involved removing the entire lens and its attachments from the ciliary body. Patients were kept in the hospital for bed rest for approximately one week after the surgery.
Because this technique was used before IOLs became available, the lens that was removed was not replaced. To see clearly after surgery, very thick glasses with a large magnifying effect (commonly known as “coke bottle” glasses) were used.
These glasses were difficult to adjust to and many people had problems moving about, especially on uneven surfaces and or in new areas. Following surgery, patients had to lie still in bed while the eye healed, often with sandbags around their head to keep them from moving. With the development of better sutures (stitches), patients were released after a few days and their activities were less restricted.
Several advancements have dramatically improved cataract surgery from the days of ICCE. These include the development of replacement lenses and agents known as viscoelastics.
Extra-capsular cataract extractionExtra-capsular cataract extraction (ECCE) refers to surgery in which the entire cataract is removed through an opening made in the anterior lens capsule. The rest of the lens capsule and all its attachments are left intact.
Most cataracts have a diameter of at least 10mm. Therefore, an incision (cut) of at least this length is to be made to remove the cataract. The new lens, usually a PC IOL, is then placed in the lens capsule.At the end of the procedure, many tiny sutures (stitches) are needed to close the wound.
This procedure became very successful because patients could have surgery and go home the same day. However, because of the large incision, this procedure caused several problems. Many patients took longer to heal and to regain the ability to carry out daily activities. Eventually a new procedure that reduced the size of the incision was developed
These two techniques are not used much anymore except in special cases.
PhacoemulsificationIt is a procedure in which the nucleus is broken down into smaller pieces within the bag and removed. Ultrasonic energy is used to emulsify the lens material. It requires a very small incision; hence the healing is much faster with less postoperative astigmatism. A foldable lens can be inserted through the small incision. The technique is also much safer than other methods.
SiliconesThey are odorless, colourless, water resistant, chemical resistant, and oxidation resistant, stable at high temperature, and do not conduct.
The cataract has the shape of a small magnifying lens and is about the size of the nail on your little finger (approximately 13mm). The lens of the eye is covered by a very fine, thin, clear membranous lens capsule. The lens capsule is attached to the inside of the eye, just behind the iris by very fine attachments known as zonules. These zonules hold the lens in place and control its ability to focus.
Inside the capsule, the lens material is made of two components: soft material called the cortex and harder central material called the nucleus. In many ways, the lens of the eye is like a peach or cherry; the outside skin is the capsule, the pulp is the cortex and the pit is the nucleus.
Intraocular lensThis is an artificial lens which is placed in the eye after surgical removal of the cataract (Opacified natural lens of the eye). Over the years there has been a marked improvement in the manufacture and design of IOLs. The basic design of an IOL consists of a central optic with haptics.
OpticIt is the central portion which refracts the light entering the eye. It can be plano convex or biconvex.
HapticsThese are the appendages attached to the optic to keep it in place. They may have various designs, like J loop, C loops, plate etc. An IOL can be placed in different positions in the eye:
- - Posterior chamber – The IOL is placed within the capsular bag, or in the sulcus
- - Anterior chamber – The IOL is placed in the anterior chamber over the iris
- - Iris fixated – These IOLs are placed in the pupillary space and attached to the iris
- - Scleral fixated – These IOLs are placed behind the iris and the haptics are sutured to the sclera
-
a. Rigid (Requires a large incision)
b. Foldable (Requires a smaller incision for insertion as these lenses are flexible) -
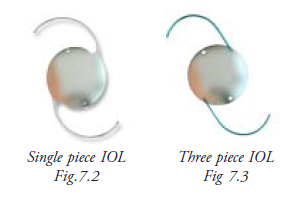
a. Single piece: Haptic and optic are made of the same material and are an integral part of the IOL (Fig. 7.2)
b. Three pieces - Haptics and optics are made of different material. (Fig. 7.3)
The haptics are then attached to the optic. Thus the IOL has 3 pieces - 1 Optic and 2 Haptics. Haptics are attached to the optic by fusion.
IOLs are made of different materials:- - PMMA - Rigid IOLs are made of PMMA
- - Silicon - used to make foldable IOLs. They are chemically inert, thermally stable and resistant to oxidation.
- - Hydrogel - resistant to degradation and oxidation and can withstand sterilisation used to make foldable IOLs. They are very flexible, cause less damage to corneal endothelium and are autoclavable.
- - Flexible acrylics are also used in foldable IOLs . They have a higher refractive index and require a controlled unfolding. They are less likely to be damaged by the YAG laser
- - Polyamide
- - Dacron
- - Mersilens
- - Polypropylene
- - PMMA
If the power of the lens is less than zero that is -1, -2, -3 etc. it is called a negative power lens.
Visco elasticsThese are jelly like substances used during ocular surgery.
- - Maintain the anterior chamber
- - Protect structures like corneal endothelium and iris from surgical trauma
- - Give the surgeon a better view
Two commonly used visco elastics are viscoat and healon.
SummaryIn this unit the OA learns the different types of sutures, needles, lenses and their uses. It helps them to identify the appropriate type and hand over the required lens to the surgeon.
Key points to remember- - There are several types of IOLs used in cataract surgery
- - Price of the lenses may vary but the outcome will be similar
- - Sutures are made of different materials
- - Sutures are available with a variety of needles already attached
I. Answer the following
- Write a short note on:
- Sutures and needles
- Non-absorbable sutures
- Needles
- IOLs are made of different materials. What are the materials used?