Low Vision Aids
Introduction
For a patient with low vision, the ophthalmologist’s positive attitude towards rehabilitation assures the patients that problems presented by sight loss can be managed. They encourage patients to use the remaining vision they have to enhance the quality of their lives. It is a time-consuming process, but to watch a person move from hopelessness and dependence to self-respect and independence is inspiring.
Low Vision
Definition
A person with low vision is one who has impairment of visual functioning even after treatment, surgery or standard refractive correction and has a visual acuity of less than 6/18, –or a field of less than 10 degrees from the point of fixation in the better eye.
Ocular conditions causing low vision
- Albinism
- High myopia
- Diabetic retinopathy
- Macular degeneration
- Micro ophthalmus.
- Early stage of retinitis pigmentosa
- Aniridia
- Corneal degeneration
Conditions where there is not much benefit from low vision devices are patients who have a visual acuity of less than 2/60 or a field of less than 10 degrees.
Advanced retinitis pigmentosa with tubular fields
Advanced glaucoma
Conditions with irreversible blindness
Optics of LVA
The image formed using hand magnifier is at infinity and the emerging rays passing through a hand magnifier is parallel and makes a point source in retina. So a patient using a hand magnifier can use it without a bifocal addition glass.
Stand magnifier: In a stand magnifier the image formed is before infinity and the rays are diverging. So a bifocal addition is necessary.
Low Vision Optical Devices
The low vision optical devices provide a magnified view of objects. They consist of the following:
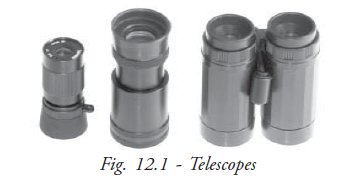
Telescopes
They are prescribed for viewing distant objects at optical infinity (Fig. 12.1). They are available as hand held or spectacle mounted, monocular or binocular. They can be manually adjusted or auto focus.
Hand magnifier
There is a large variety of hand held magnifiers available with different features such as aspheric surfaces, illumination, multiple lenses that can be combined to alter the total power, and a protective shield to house the lens when not in use (Fig. 12.2).
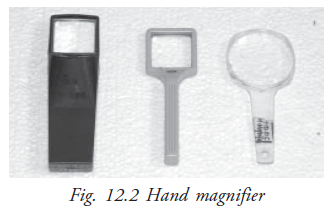
It is a conventional familiar aid, which can be used along with the distance glasses or without glasses. The lens can be held against a spectacle lens with one hand. They are very cost effective, portable and useful for short term reading tasks.
Those who have limited dexterity or hand tremors cannot use it, and it is also difficult to use for prolonged period.
Stand magnifier
There are a large variety of stand magnifiers with different features including a clear housing, illumination and aspheric surface (Fig. 12.3). Most stand magnifiers are designed for use with a standard bifocal or reading glass. They have a fixed focus.
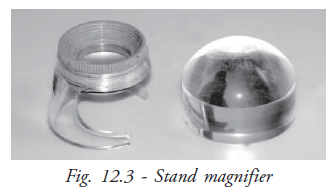
Stand magnifiers have constant magnification. They are helpful for children or patients with reduced coordination and hand tremors. But they are inconvenient to carry and may result in bad posture after prolonged use.
High-plus addition
There are large varieties of high plus spectacles available like convex sphere, aspheric sphere, aspheric lenticular, aspheric doublet, bifocal, clip-on loupes, prism sphere (Fig. 12.4a and Fig. 12.4b).
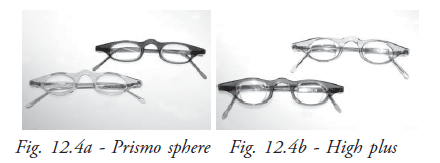
They facilitate hand work, and provide the widest field of view, greater reading speed and cosmetic acceptability.
The closer working distance can obstruct illumination. When the power is too high it makes writing difficult.
Closed circuit television
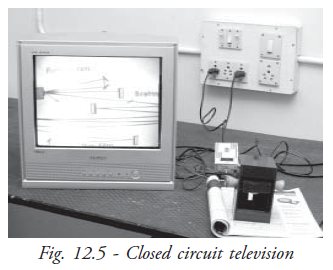
A closed circuit television (CCTV) reading system is a television camera that relays a magnified image to a monitor screen (Fig. 12.5).
They are devices that allow binocularity at high levels of magnification, at a relatively normal working distance. They allow sufficient reading speed. Magnification can be adjusted for different print sizes.
Non Optical Devices
The function of a non-optical device is to enhance the use of vision with or without optical aids (Fig. 12.6). They vary in purpose and are individualized according to the patients needs. It facilitates an environment for efficient functioning.
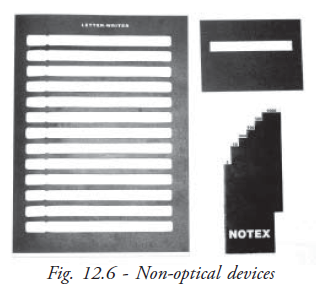
There are seven categories of devices. They are:
- Relative size or larger assistive devices
- Glare, contrast and lighting control devices
- Posture and comfort maintenance devices
- Written communication devices
- Medical management devices
- Orientation and mobility management devices
- Sensory substitution devices
Low vision Evaluation and Management
Low vision evaluation
Evaluation of the remaining visual function is a key component of low vision rehabilitation. It reveals how patients are using their vision and gives insights into adaptations they are already making use of.
Estimates of visual loss are measured by visual acuity for distance, near, contrast sensitivity, photophobia, color vision, visual fields, etc
Assessment provides for the needs of the patients for education, vocation, daily activities, mobility, social interaction, and psychological reaction, reading and writing performance.
Formulas used in deriving predicted add
Kestenbaum formula
If the patient’s best acuity is 6/60 then its reciprocal will be 60/6=1OD.
Required near vision addition will be +1O D.
The lighthouse method
The near vision acuity card is used at 40 cm distance and the patient is given a +2.5D add. Depending on the test distance up to 10cm the add can be increased. The letter size is found on the left side and dioptric add on the right side of the acuity card.
Adjustment training
The philosophy of rehabilitation is that if patients focus on their capabilities rather than on their disabilities, they can begin the process of adapting to the environment and becoming a viable part of it. The program of rehabilitation starts with the evaluation of the patient’s abilities and analysis of skills required to meet the activities of daily living.
The process begins with dependence and sense of helplessness and ends with independence and sense of self-achievement. The training instills in the patients with disability a sense of empowerment, that they have control over their lives and can make decisions for themselves.
Generally three approaches are taken in the treatment process:
- Manipulating the environment to make it user friendly
- Increasing the effective use of remaining vision
- Teaching patients to compensate with other sensory system
Counselling and guidance
Counselling and guidance play an important part in patients’ understanding. The information to be delivered through counselling:
- The name of the disease or condition, the part of the eye or brain that is affected
- The functional implication of the condition, visual acuity contrast sensitivity, visual fields, and any other clinical evaluation
- The refractive error and why the former prescription is no longer helpful
- The recommended device and how it assists in completing desired activities of daily living
- Illumination needs, preferences and problems, both indoors and out doors
- Instruction without devices to help maximize visual abilities: Fixation, eccentric viewing, scotoma awareness, scanning, spotting etc
- Instruction with devices
- The psychosocial implication of visual loss
A lot of “home work” or practice increases the visually challenged patients’ ability to reach their goals
Student exercise
Answer the following
- Define low vision
- What are the causes of low vision?
- What are the types of devices given for low vision patients?
- Explain about the stand magnifier
- How do you counsel a low vision patient?
- Write the formula for predicting “the add”